Deep melodic house as a multi-domain non-pharmacological wellbeing intervention. A clinical synthesis of music neuroscience evidence, organised into a four-pathway model with applications across eight clinical domains.
Music sits in an unusual place in modern healthcare
Almost every patient already uses it. Few clinicians prescribe it. The evidence base, however, has matured considerably.
What's been missing is genre-specific reasoning. Most clinical work has used classical music or generic relaxation tracks selected for tempo alone. Adherence suffers, particularly in patients under fifty. The premise of this framework is that one specific subgenre, deep melodic house, possesses an acoustic signature that aligns more precisely with the music characteristics shown to drive therapeutic outcomes than the standard repertoire used in research, while remaining culturally accessible and emotionally engaging in a way that supports adherence.
01 · What we know
Music drives measurable change
Meta-analyses report medium-to-large effects on stress (d ≈ 0.72), medium effects on anxiety (g ≈ 0.36), and clinically meaningful improvements in sleep (PSQI MD ≈ -3.4) and ADHD executive function (SMD ≈ 0.45-0.50).
02 · What's missing
Genre-specific reasoning
Almost no published trials use contemporary electronic music. The acoustic features that make music therapeutic, however, are properties of sound, not of genre. Deep melodic house has them.
03 · What we propose
A four-pathway clinical model
An evidence-grounded, mechanism-explicit framework that maps acoustic features through four pathways to outcomes across eight clinical domains, with a usable protocol and implementation pathway.
The genre in pictures
The culture
Translating clinical evidence into clinical practice means understanding what the music actually feels like, who plays it, where it lives. The framework is grounded in the music's cultural reality. The visual essay below shows the spectrum, from solo immersion to mass listening, from a sunset rooftop set to an underground club, from a focused listener at home to a euphoric crowd. Each image ties to one or more of the four pathways the framework identifies.
Mass listening at scale. The socio-behavioural pathway in action: shared parasympathetic shift, identity, ritual, belonging.
Cognitive-affective
The listener as patient. Solo immersion is the most common mode of engagement and the simplest delivery channel.
Neuroendocrine
The Mood Lift profile, embodied. Sunset sets pair the genre's emotional register with light movement and warm light.
Cognitive-affective
Receptive listening, the protocol's primary mode. Headphones, focused attention, no external performance.
Cognitive-affective
Performer flow. Concentration without sympathetic arousal, the cognitive-affective pathway in its purest state.
Socio-behavioural
The underground. Intimate community, shared identity, ritual, the socio-behavioural pathway at its most concentrated.
Neuroendocrine
Joy without ecstasy. The genre's signature emotional register, reward without spike-and-crash.
Autonomic
The vehicle. High-quality over-ear headphones substantially enhance therapeutic effect through low-frequency reproduction and environmental masking.
Socio-behavioural
The DJ as facilitator. Collective parasympathetic shift in shared space, what music neuroscience calls 'group entrainment'.
Socio-behavioural
Visual identity. The genre's lineage to a distinct aesthetic vocabulary supports community belonging and adherence.
The framework at a glance
Six domains, one acoustic signature
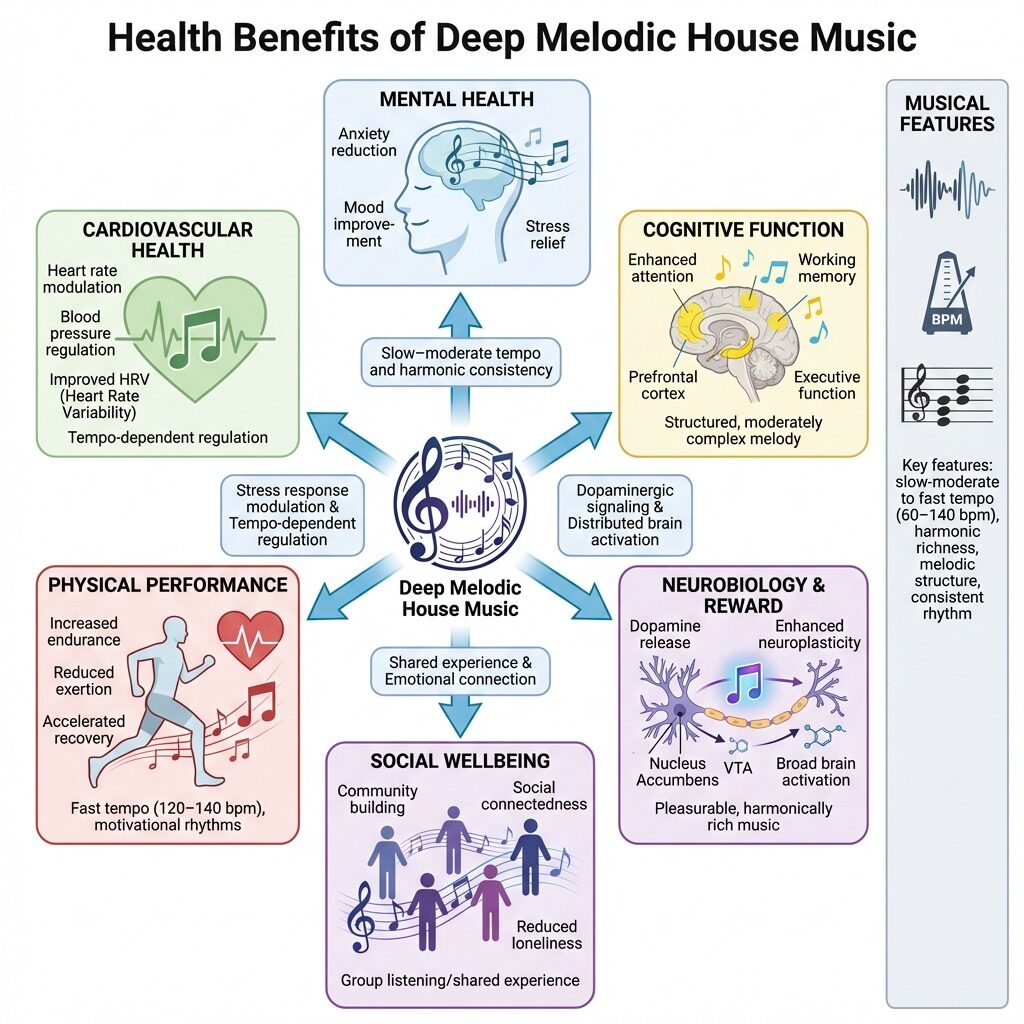
The diagram below summarises how the genre's core musical features (slow-to-moderate tempo, harmonic richness, melodic structure and consistent rhythm) connect through neurobiology and reward to the broader categories of mental health, cognitive function, cardiovascular health, physical performance, social wellbeing and reward. Each downstream domain is explored in detail later on the page.
Figure 1. The Sanctum Resonance Framework at a glance. Click to enlarge.
The acoustic signature
Seven elements that make this genre therapeutic
Deep melodic house has a defined acoustic profile. Each element below maps onto a documented therapeutic mechanism. Click any element to explore why it matters clinically.
Mechanism
The four pathways
The framework identifies four interlocking pathways through which deep melodic house's acoustic features drive physiological, psychological and behavioural change. Each card below shows the acoustic driver, the mechanism and the primary outcomes. Click any card to read more.
Application
Eight clinical domains
The four pathways deliver effects across the eight domains below. Effect sizes are drawn from meta-analyses where available, individual high-quality trials otherwise. Filter by pathway to see which domains each engages most strongly.
Evidence at a glance
Effect sizes across domains
Effect sizes are typically small to medium for stand-alone music interventions, growing to medium-to-large when music is combined with movement, mindfulness or cognitive elements. The chart below shows the most important meta-analytic effects, scaled for visual comparison.
Stress (d = 0.72)
0.72
Anxiety (g = 0.41)
0.41
Depression (HAMD -41%)
0.85
Sleep (PSQI -3.37)
0.62
ADHD / EF (SMD 0.50)
0.50
CV / Inflammation
0.55
Pain (SMD 0.42)
0.42
Menstrual / Menopausal
0.86
Addiction
0.30
Strong evidence (multiple meta-analyses)
Moderate evidence
Emerging evidence
Clinical protocol
From framework to clinic
Five elements turn the framework into a useable protocol. Each tab below covers one element. The protocol is a starting point, local adaptation is expected.
Strongest indications
Adults and adolescents with mild-to-moderate anxiety, work-related or study-related stress, mild depression with prominent rumination or anxiety features, ADHD where executive function and emotional regulation are problematic, sleep onset difficulty (with appropriate pre-sleep timing), perimenopausal symptom complex, dysmenorrhoea, chronic pain conditions where catastrophising contributes to symptom severity, and individuals in early to mid recovery from substance use disorders. Also suitable as a wellbeing maintenance tool for asymptomatic individuals.
Caution
In patients with severe mental illness, particularly active psychosis, sustained sensory input may be problematic. Caution is also warranted in individuals whose music history is closely entangled with substance use of a specific genre.
Four listening profiles
Not all deep melodic house is therapeutically equivalent. Three sub-categories within the genre serve different clinical purposes, plus a movement-oriented variant. Each profile's image cues the listening context.
110 to 118 BPM
Deep Calm
Slow, atmospheric, designed for parasympathetic shift. Strongest for sleep difficulty, anxiety with rumination, evening wind-down.
Artists: Lane 8, Tinlicker, Marsh, Yotto (slower), Bonobo
118 to 122 BPM
Focus and Regulation
Steady, grounded, the cardiopulmonary focus zone. Strongest for ADHD, daytime stress, work and study, mild anxiety.
Artists: Ben Böhmer, Tinlicker (energetic), Eli & Fur, Kasablanca
122 to 125 BPM
Movement and Energy
Driving steady kick with emotional engagement. Strongest for ADHD with hyperactivity, exercise motivation, low mood with reduced activity.
Artists: RÜFÜS DU SOL, CamelPhat, Hot Since 82, Cassian (energetic)
Physical performance benefits
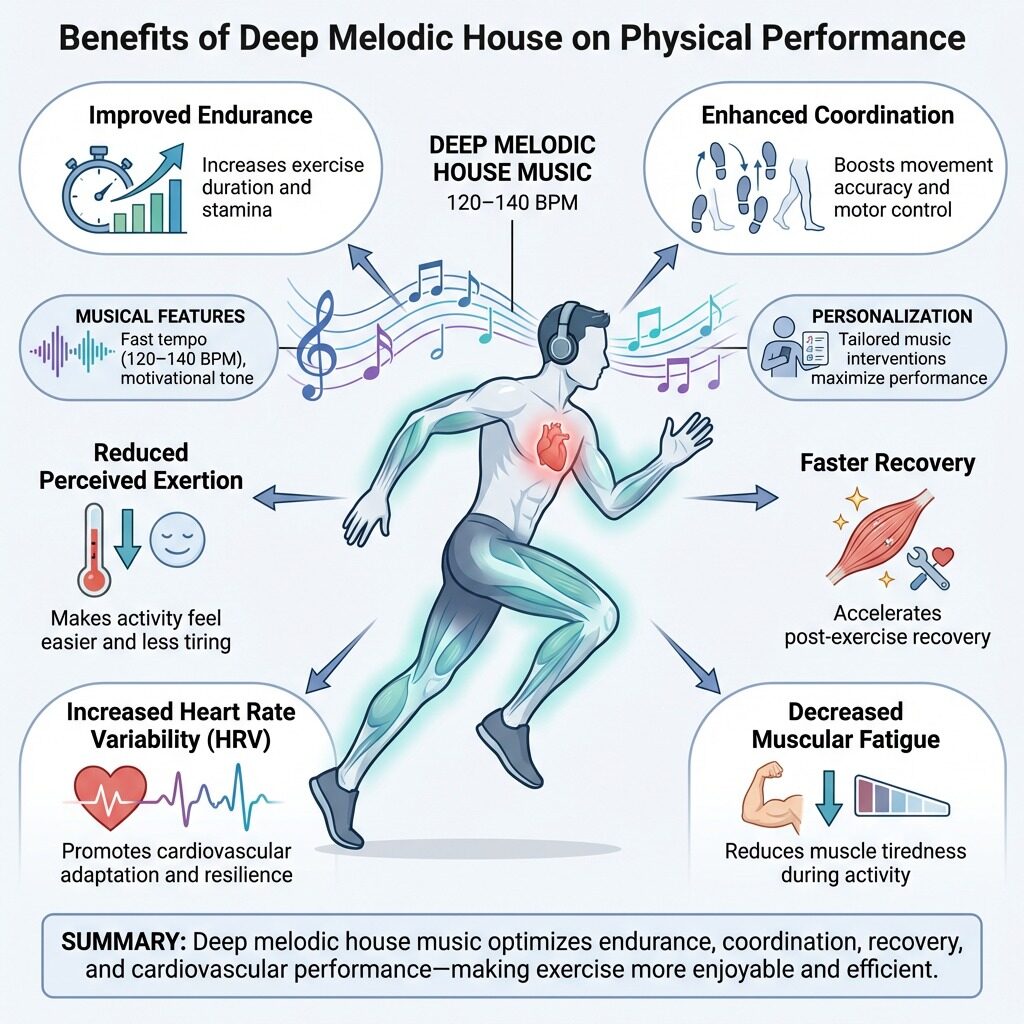
For the Movement profile, music-assisted exercise produces measurable benefits across endurance, coordination, perceived exertion, recovery, heart rate variability and muscular fatigue. The diagram below summarises the mechanisms.
Physical performance benefits of deep melodic house in the 120 to 140 BPM zone.
What to avoid
Tracks with abrupt drops, aggressive distortion, peak-time intensity, semantic-rich lyrical content (which competes for cognitive resources) and sudden dynamic changes. These break parasympathetic states and can trigger the orienting response.
Acute exposure
20 to 45 minutes is the canonical session length, supported by multiple trials. The He (2026) sleep meta-analysis identified 30 to 45 minute sessions, four to eight weeks duration as optimal for sleep quality. The de Witte stress meta-analysis showed effects across a range of session lengths from 15 to 60 minutes.
Frequency and duration
Daily exposure during a symptomatic phase, or three to seven sessions weekly for general wellbeing maintenance, are both well-supported. Sustained benefits typically require four to twelve weeks of regular use. The Li and Min (2024) trauma study showed a clear dose-response relationship, with patients attending more than 20 sessions experiencing 33.6 percent positive outcomes.
Delivery
High-quality headphones substantially enhance effectiveness through environmental masking, immersion and the reproduction of low-frequency content critical to the genre. Open-back headphones for waking activities, in-ear monitors for portable use, sleep-specific headphones for through-the-night listening.
Hearing health
Headphone use should be avoided during activities requiring environmental awareness (driving, cycling, walking in traffic). Volume should be kept at moderate levels, particularly during extended listening sessions.
Medical considerations
Patients with tinnitus may find sustained low-frequency content uncomfortable, brief trial exposure is advised. In severe mental illness, particularly conditions with auditory hallucinations or paranoid features, music interventions should be supervised by mental health professionals. In acute trauma, content selection should be careful, warm grounding bass is generally preferable to highly emotional vocal-led tracks.
Adjunctive use, not replacement
The framework positions deep melodic house as adjunctive to standard care, not a substitute for first-line treatment. Patient education should be explicit on this point to mitigate opportunity-cost risk.
Three parameters that matter
1. Baseline arousal state
Patients in a hyperaroused state benefit from slower tempo (110 to 118 BPM) initially, with potential gradual increase. Patients in a hypoaroused state, including some depression presentations, may benefit from the upper range (122 to 125 BPM).
2. Individual heart rate
The Motokawa and Kato (2025) vibration-and-music work showed greatest cortisol reduction in participants whose heart rates matched intervention tempo. Heuristic: select tempo within five to ten BPM of the patient's resting heart rate, then move towards the lower end as the session progresses.
3. Listener preference
Participant-selected music outperforms standardised music for HRV improvements (Zhang 2026). Within the genre's broad parameters, allowing patients to select tracks and artists they prefer enhances adherence and outcomes.
Implementation
Five tiers, from self-directed to AI-driven
The framework can be implemented at several levels of intensity. Each tier carries different resource, training and infrastructure requirements. Click any tier to expand.
Try the screening tool
The Sanctum Resonance screen is a five-minute patient-facing instrument that maps presenting symptoms to one of the four listening profiles, with specific artist recommendations and direct streaming links.
Honest accounting of what we don't yet know is essential. The evidence base supporting this framework is broad but has clear limitations, and the priority research questions follow directly.
Priority 01
Genre-specific RCTs
No published controlled trials have used deep melodic house specifically. Almost all evidence is extrapolated from research using classical music or unspecified relaxation music. Direct genre comparisons are needed across stress, anxiety, sleep and ADHD populations.
Priority 02
Dose-response curves
Optimal dosing for specific outcomes remains under-characterised. Trauma data suggest dose-response continues past 20 sessions, but the curve has not been mapped. Systematic variation of session length, frequency and total duration is needed.
Priority 03
Personalisation algorithms
Wearable HRV, listener preference and baseline arousal state likely outperform standardised protocols. Adaptive AI-driven systems show early promise but require robust validation in clinical populations.
Priority 04
Mechanism characterisation
Direct fMRI and PET studies of mesolimbic and prefrontal activity during deep melodic house listening. Pharmacological probes to confirm mediating roles of dopamine and endogenous opioids. Inflammatory marker studies to test the predicted vagal-anti-inflammatory pathway.
Priority 05
Combination interventions
Music plus movement, music plus mindfulness, music plus CBT, music plus standard pharmacological care. Synergistic effects are predicted by the framework but require systematic testing.
Priority 06
Real-world implementation
Feasibility, acceptability, adherence, cost-effectiveness and integration with existing UK NHS and community care pathways. Implementation research bridges the gap between mechanism and routine practice.
References
Selected bibliography
A selective, searchable list of the principal sources informing the framework.